Equity Through Engagement
Children in Medi-Cal Are Being Left Behind
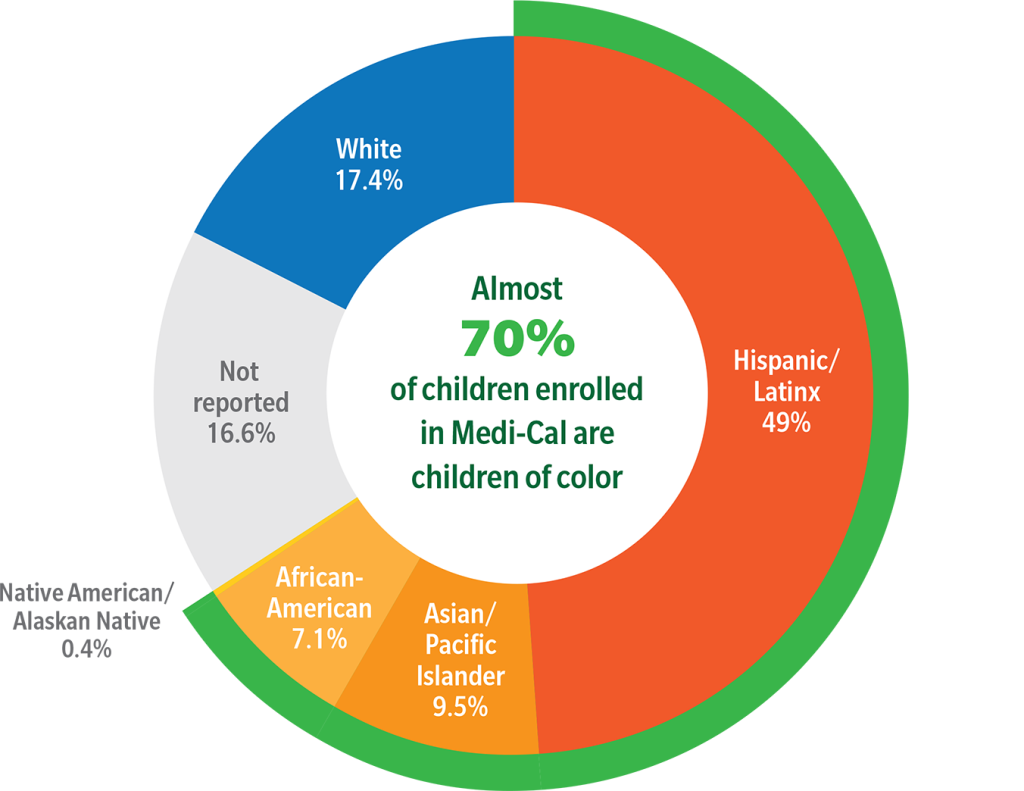
Medi-Cal Enrolled Children by Race/Ethnicity, January 2022
Medi-Cal insures more than 5 million children—nearly 60% of all children in California, and is the primary form of coverage for Black and Latinx children.
We rank in the lowest 10% of states for providing critical early behavioral, social, and developmental screenings, and 48th in the nation in access to mental health services for children.
California does not spend what it would take to meet the needs of children. Only 14% of Medi-Cal expenditures are on children, yet they represent nearly 40% of all beneficiaries.
At its core, this is an equity issue. Almost 70% of children in Medi-Cal are children of color and they are not coming close to getting what they need or are entitled to in the program.
Managed Care Plans Are Responsible for Advancing Children’s Health Equity
Almost all children in Medi-Cal (92%) get their care delivered through a public or private Managed Care Plan (MCP), making MCPs the central player in how vulnerable youth and their families are served.
For our most vulnerable children to have equitable healthcare outcomes MCPs must ensure children receive the healthcare they need, in a place that is safe and comfortable for them and their families, and from someone who is personally familiar with the unique healthcare needs of their cultural background.
For this to happen the state must hold MCPs accountable for:
- Setting a guaranteed minimum spend on children’s physical and mental health care and being transparent about their investments and expenditures.
- Providing proactive, preventive services which by definition do not require a diagnosis.
- Expanding and sustaining provider classes that proliferate social, peer-based, and mutual aid models.
- Investing in community partners to change policies, laws, and regulations that improve community conditions (social drivers of health) and ensure health for all children.
- Shifting power in the system by actively and genuinely engaging families in defining, developing, and delivering children’s health care services.
The Equity Through Engagement (ETE) project is a partnership of The Children’s Partnership, The Georgetown Center on Poverty and Inequity, and California Children’s Trust to advance child health equity in California. ETE examines opportunities for Medi-Cal managed care to better partner with community collaboratives, community based organizations and families to advance child health equity.
The ETE project produced the following materials to illustrate how these areas of focus can advance child health equity.

REIMAGINING MEDI-CAL: Collaborating with Families and Communities to Advance Child Health Equity
In this final report of the Equity Through Engagement (ETE) project, we examine MCPs as a tool to advance child health equity by looking at the extent to which they can play a central role in Medi-Cal responding to social drivers of health and health-related social needs for children’s health. We also explore how communities and families, as experts in their own needs, can be better centered in the equation between health care systems and child health equity.
- Executive Summary (September 2022)
- Full Report (September 2022)

Families Must Be Partners in Reimaging Medi-Cal for Children’s Health Equity
Our Family Voices Matter report, and accompanying executive summary and family voices snapshot, confirmed the urgent need for MCPs to better partner with families as an essential step toward improving children’s mental health equity.
- Full Report: Listening to the Real Experts in Medi-Cal Children’s Health (July 2022)
- Executive Summary (July 2022)
- Family Voices Snapshot (July 2022)

Care Coordination Is Essential to Children Accessing the Care They Need
In our care coordination reports we: 1) look at the obligations of MCPs to provide care coordination for all children in Medi-Cal, 2) present successful children’s care coordination models and examples of care coordination in action, and 3) make recommendations for how MCPs can improve care coordination to ensure children receive the preventive and ongoing healthcare.

Data Helps Identify Focus Areas for Improving Child Health Equity
The Child Opportunity Workbook uses Child Opportunity Index (COI) scores developed by Brandeis University and the Ohio State University to assess social drivers of health by race and county across California. It provides policymakers and advocates interested in improving child health care equity with a useful snapshot of disparities in opportunity across California.
We are honored to have completed the Equity Through Engagement project with the following partners:
![]()
The Children’s Partnership (TCP) is a California advocacy organization advancing child health equity through research, policy and community engagement. We envision a California where all children—regardless of their race, ethnicity or place of birth—have the resources and opportunities they need to grow up healthy and thrive. For more information, visit The Children’s Partnership website.

The Georgetown Center on Poverty and Inequality (GCPI) works with policymakers, researchers, practitioners, advocates, and people with lived experience to develop effective policies and practices that alleviate poverty and inequality in the United States. The mission of GCPl’s Economic Security and Opportunity Initiative (ESOI) is to expand economic inclusion in the United States through rigorous research, analysis, and ambitious ideas to improve programs and policies. For more information, visit the Georgetown Center website.